By decreasing the interval periods and increasing the frequency of exercise bouts, we were able to confirm our hypothesis that middle-aged adults could achieve a greater reduction in arterial stiffness through intermittent exercise. Thirty middle-aged males were randomly divided into a control group (CON), continuous exercise group (CE), interval exercise long-long group (IELL), interval exercise long-short group (IELS), and interval exercise short-short group (IESS). The subjects performed moderate-intensity exercise on the treadmill. Cardio-ankle vascular index (CAVI) was assessed before exercise, right after the session ended, and at 30 and 60 minutes into the recovery period. Changes in values from the baseline (∆CAVI) during each measurement were used for analysis. The control group showed no significant change in ∆CAVI, while all exercise groups showed a significant decrease at 0, 30, and 60 minutes. The exercise groups had significantly lower ∆CAVI than the control group at 0 and 30 minutes. At 60 minutes, the IESS group had a significantly lower ∆CAVI than the control group. Additionally, at 0 and 30 minutes, the IELS and IESS groups had a significantly lower ∆CAVI than the CE group. Hence, interval exercise is more effective than continuous exercise regardless of the total duration, but the effectiveness depends on the interval duration and number of repetitions.
| Published in | International Journal of Sports Science and Physical Education (Volume 9, Issue 4) |
| DOI | 10.11648/j.ijsspe.20240904.15 |
| Page(s) | 79-86 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Interval Exercise, Arterial Stiffness, Middle-Aged, Cardiovascular Disease
Value (Mean ± SE) | |
|---|---|
Age (years) | 56.5 ± 1.9 |
Height (cm) | 171.2 ± 4.3 |
Weight (kg) | 80.3 ± 5.3 |
BMI (kg/m2) | 27.2 ± 5.7 |
Systolic BP (mmHg) | 132.3 ± 3.5 |
Diastolic BP (mmHg) | 81.8± 2.7 |
CAVI | 8.2± 0.6 |
CVD | Cardiovascular Disease |
CAVI | Cardio-ankle Vascular Index |
PWV | Pulse Wave Velocity |
BMI | Body Mass Index |
| [1] | Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J 2006; 27: 2588-605. |
| [2] | Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol 2010; 55: 1318-27. |
| [3] | Mitchell GF, Hwang SJ, Vasan RS, Larson MG, Pencina MJ, Hamburg NM, Vita JA, Levy D, Benjamin EJ. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation 2010; 121: 505-11. |
| [4] | Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, Ducimetiere P, Benetos A. Aortic stiffness is an in-dependent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001; 37: 1236-41. |
| [5] | Vlachopoulos C, Aznaouridis K, Terentes-Printzios D, Ioakeimidis N, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with brachial-ankle elasticity index: a systematic review and meta-analysis. Hyper-tension 2012; 60: 556-62. |
| [6] | Blacher J, Asmar R, Djane S, London GM, Safar ME. Aortic pulse wave velocity as a marker of cardiovascular risk in hypertensive patients. Hypertension 1999; 33: 1111-7. |
| [7] | Shirai K, Utino J, Otsuka K, Takata M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J Atheroscler Thromb 2006; 13: 101-7. |
| [8] | Koshiba H, Maeshima E. Effects of exercise intervention on arterial stiffness in middle-aged and older females: evaluation by measuring brachial-ankle pulse wave velocity and cardio-ankle vascular index. J Phys Ther Sci 2019; 31: 88-92. |
| [9] | Heil L, Oberhoffer R, Bohm B. Association Between Physical Activity Intensity Levels and Arterial Stiffness in Healthy Children. J Phys Act Health 2020; 17: 933-9. |
| [10] | Higaki Y, Yamato Y, Fujie S, Inoue K, Shimomura M, Kato S, Horii N, Ogoh S, Iemitsu M. Acute effects of the differ-ent relaxation periods during passive intermittent static stretching on arterial stiffness. Plos One 2021; 16: e259444. |
| [11] | Zhou Z, Hou L, Cui M, Mourot L, Zhu W. Acute effects of low-volume intermittent versus higher-volume continuous exercise on arterial stiffness in healthy young men. Sci Rep 2022; 12. |
| [12] | Trapp EG, Chisholm DJ, Freund J, Boutcher SH. The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. Int J Obes (Lond) 2008; 32: 684-91. |
| [13] | Trapp EG, Chisholm DJ, Boutcher SH. Metabolic response of trained and untrained women during high-intensity intermittent cycle exercise. Am J Physiol Regul Integr Comp Physiol 2007; 293: R2370-5. |
| [14] | Tordi N, Mourot L, Colin E, Regnard J. Intermittent versus constant aerobic exercise: effects on arterial stiffness. Eur J Appl Physiol 2010; 108: 801-9. |
| [15] | Peres D, Mourot L, Ménétrier A, Bouhaddi M, Degano B, Regnard J, Tordi N. Intermittent versus constant aerobic exercise in middle-aged males: acute effects on arterial stiffness and factors influencing the changes. Eur J Appl Physiol 2018; 118: 1625-33. |
| [16] | Perissiou M, Bailey TG, Windsor M, Nam M, Greaves K, Leicht AS, Golledge J, Askew CD. Effects of exercise intensity and cardiorespiratory fitness on the acute response of arterial stiffness to exercise in older adults. Eur J Appl Physiol 2018; 118: 1673-88. |
| [17] | Ren J, Xiao H, Wang P. Acute Effects of the Interval and Duration of Intermittent Exercise on Arterial Stiffness in Young Men. International Journal of Environmental Research and Public Health 2022; 19: 16847. |
| [18] | Sardeli AV, Gáspari AF, Chacon-Mikahil MP. Acute, short-, and long-term effects of different types of exercise in central arterial stiffness: a systematic review and meta-analysis. The Journal of Sports Medicine and Physical Fitness 2018; 58. |
| [19] | Hortmann K, Boutouyrie P, Locatelli JC, de Oliveira GH, Simões CF, de Souza Mendes VH, Reck HB, Okawa RTP, Lopes WA. Acute effects of high-intensity interval training and moderate-intensity continuous training on arterial stiffness in young obese women. Eur J Prev Cardiol 2021; 28: e7-10. |
| [20] | Lopes S, Afreixo V, Teixeira M, Garcia C, Leitão C, Gouveia M, Figueiredo D, Alves AJ, Polonia J, Oliveira J, Mes-quita-Bastos J, Ribeiro F. Exercise training reduces arterial stiffness in adults with hypertension: a systematic review and meta-analysis. J Hypertens 2021; 39: 214-22. |
| [21] | Hu J, Liu M, Yang R, Wang L, Liang L, Yang Y, Jia S, Chen R, Liu Q, Ren Y, Zhu L, Cai M. Effects of high-intensity interval training on improving arterial stiffness in Chinese female university students with normal weight obese: a pilot randomized controlled trial. J Transl Med 2022; 20: 60. |
| [22] | Siasos G, Athanasiou D, Terzis G, Stasinaki A, Oikonomou E, Tsitkanou S, Kolokytha T, Spengos K, Papavassiliou AG, Tousoulis D. Acute effects of different types of aerobic exercise on endothelial function and arterial stiffness. Eur J Prev Cardiol 2016; 23: 1565-72. |
| [23] | Krankel N, Bahls M, Van Craenenbroeck EM, Adams V, Serratosa L, Solberg EE, Hansen D, Dorr M, Kemps H. Exercise training to reduce cardiovascular risk in patients with metabolic syndrome and type 2 diabetes mellitus: How does it work? Eur J Prev Cardiol 2019; 26: 701-8. |
| [24] | Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, Nieman DC, Swain DP. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 2011; 43: 1334-59. |
| [25] | Zheng L, Zhang X, Zhu W, Chen X, Wu H, Yan S. Acute effects of moderate-intensity continuous and accumulated exercise on arterial stiffness in healthy young men. Eur J Appl Physiol 2015; 115: 177-85. |
| [26] | Zhou Z, He Z, Yuan M, Yin Z, Dang X, Zhu J, Zhu W. Longer rest intervals do not attenuate the superior effects of accumulated exercise on arterial stiffness. Eur J Appl Physiol 2015; 115: 2149-57. |
APA Style
Xiao, H., Ren, J. (2024). Optimizing Exercise Interval for Arterial Stiffness Improve-Ment in Middle-Aged Adults. International Journal of Sports Science and Physical Education, 9(4), 79-86. https://doi.org/10.11648/j.ijsspe.20240904.15
ACS Style
Xiao, H.; Ren, J. Optimizing Exercise Interval for Arterial Stiffness Improve-Ment in Middle-Aged Adults. Int. J. Sports Sci. Phys. Educ. 2024, 9(4), 79-86. doi: 10.11648/j.ijsspe.20240904.15
AMA Style
Xiao H, Ren J. Optimizing Exercise Interval for Arterial Stiffness Improve-Ment in Middle-Aged Adults. Int J Sports Sci Phys Educ. 2024;9(4):79-86. doi: 10.11648/j.ijsspe.20240904.15
@article{10.11648/j.ijsspe.20240904.15,
author = {Haili Xiao and Jianchang Ren},
title = {Optimizing Exercise Interval for Arterial Stiffness Improve-Ment in Middle-Aged Adults
},
journal = {International Journal of Sports Science and Physical Education},
volume = {9},
number = {4},
pages = {79-86},
doi = {10.11648/j.ijsspe.20240904.15},
url = {https://doi.org/10.11648/j.ijsspe.20240904.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijsspe.20240904.15},
abstract = {By decreasing the interval periods and increasing the frequency of exercise bouts, we were able to confirm our hypothesis that middle-aged adults could achieve a greater reduction in arterial stiffness through intermittent exercise. Thirty middle-aged males were randomly divided into a control group (CON), continuous exercise group (CE), interval exercise long-long group (IELL), interval exercise long-short group (IELS), and interval exercise short-short group (IESS). The subjects performed moderate-intensity exercise on the treadmill. Cardio-ankle vascular index (CAVI) was assessed before exercise, right after the session ended, and at 30 and 60 minutes into the recovery period. Changes in values from the baseline (∆CAVI) during each measurement were used for analysis. The control group showed no significant change in ∆CAVI, while all exercise groups showed a significant decrease at 0, 30, and 60 minutes. The exercise groups had significantly lower ∆CAVI than the control group at 0 and 30 minutes. At 60 minutes, the IESS group had a significantly lower ∆CAVI than the control group. Additionally, at 0 and 30 minutes, the IELS and IESS groups had a significantly lower ∆CAVI than the CE group. Hence, interval exercise is more effective than continuous exercise regardless of the total duration, but the effectiveness depends on the interval duration and number of repetitions.
},
year = {2024}
}
TY - JOUR T1 - Optimizing Exercise Interval for Arterial Stiffness Improve-Ment in Middle-Aged Adults AU - Haili Xiao AU - Jianchang Ren Y1 - 2024/12/09 PY - 2024 N1 - https://doi.org/10.11648/j.ijsspe.20240904.15 DO - 10.11648/j.ijsspe.20240904.15 T2 - International Journal of Sports Science and Physical Education JF - International Journal of Sports Science and Physical Education JO - International Journal of Sports Science and Physical Education SP - 79 EP - 86 PB - Science Publishing Group SN - 2575-1611 UR - https://doi.org/10.11648/j.ijsspe.20240904.15 AB - By decreasing the interval periods and increasing the frequency of exercise bouts, we were able to confirm our hypothesis that middle-aged adults could achieve a greater reduction in arterial stiffness through intermittent exercise. Thirty middle-aged males were randomly divided into a control group (CON), continuous exercise group (CE), interval exercise long-long group (IELL), interval exercise long-short group (IELS), and interval exercise short-short group (IESS). The subjects performed moderate-intensity exercise on the treadmill. Cardio-ankle vascular index (CAVI) was assessed before exercise, right after the session ended, and at 30 and 60 minutes into the recovery period. Changes in values from the baseline (∆CAVI) during each measurement were used for analysis. The control group showed no significant change in ∆CAVI, while all exercise groups showed a significant decrease at 0, 30, and 60 minutes. The exercise groups had significantly lower ∆CAVI than the control group at 0 and 30 minutes. At 60 minutes, the IESS group had a significantly lower ∆CAVI than the control group. Additionally, at 0 and 30 minutes, the IELS and IESS groups had a significantly lower ∆CAVI than the CE group. Hence, interval exercise is more effective than continuous exercise regardless of the total duration, but the effectiveness depends on the interval duration and number of repetitions. VL - 9 IS - 4 ER -
Institute of Sport and Health, Lingnan Normal University, Zhanjiang, China
Institute of Sport and Health, Lingnan Normal University, Zhanjiang, China
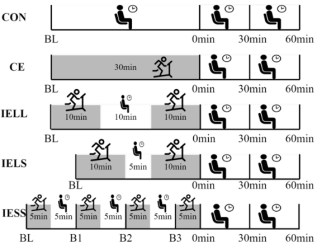
Figure 1. Exercise design. This study entails five experiments: a control experiment (CON), a single 30-minute exercise experiment (CE), two 10-minute treadmill exercise experiments with a 10-minute rest period in between (IELL), two 10-minute treadmill exercise experiments with a 5-minute rest period in between (IELS), and four 5-minute treadmill exercise experiments with a 5-minute rest period in between (IESS). In the CE, IELL, IELS, and IESS experiments, time measurements were taken at baseline (BL), immediately after exercise (0 minutes), 30 minutes after exercise, and 60 minutes after exercise. Additionally, three additional CAVI measurements were taken before the second (B1), third (B2), and fourth (B3) 5-minute exercise sessions in the IESS experiment.

Figure 2. Changes in ∆CAVI over time were observed during both intermittent exercise and continuous exercise experiments. The mean (±SD) is time-dependent ∆CAVI changes in CON, CE, and IELL trials (a) and CON, CE, and IELS trials (b). * p < 0.01, CE, IELL, and IELS vs. CON at 0 min. # p < 0.01, CE, IELL, and IELS vs. CON at 30 min. & p < 0.05, IELS vs. CE at 0 min. $p < 0.05, IELS vs. CE at 30 min. n = 30.

Figure 3. Changes in ∆CAVI over time were observed during intermittent exercise experiments with different rest periods. The mean (±SD) ∆CAVI changes in CON, CE. and IESS trials (a) and CON, IELS, and IESS trials (b). * p < 0. 01, CE, IELS, and IESS vs. CON at 0 min. # p < 0.01, CE, IELS, and IELS vs. CON at 30 min. ¥ p < 0.05, IESS vs. CON at 60 min. & p < 0.05, IESS vs. CE at 60 min. n = 30.
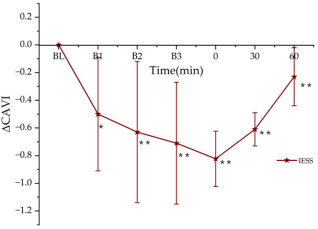
Figure 4. The change of ∆CAVI over time in the IESS experiment. * p < 0.05 vs. BL; ** p < 0.01 vs. BL. n = 30.

